


The Neonatal ICU… a paradigm of organized chaos. The moment you step inside and look around, you quickly realise its nothing like you have ever experienced before. The NICU is infact a vortex and has, in its own capacity, the power to consume you and spit you out whole. Sometimes I feel like I am being dramatic but deep down, I know I am not.
An underrated area of pure volatility and action. Every single sick baby demands an enormous amount of work to be done on them. A spectrum of disease exists in the NICU. Some babies are just passing by for observation post delivery, some preterm small babies need extra TLC to grow while fighting infections and then… the very sick type who need ventilation, blood transfuions, constant blood tests and intense monitoring. It’s like every second is life or death with you hanging in the balance.
It won’t take you long to learn never to underestimate a neonate. You turn your head or drop your pen, and in a split second, their condition has changed for the worst. Often people have this heroic perception of doctors saving lives by cutting out unwanted burst appendixes and removing rogue bullets in chests which yes, are very heroic. But in my small opinion, handling humans which are about the same weight as a block of butter takes skill, tact and a whole lot of gut.
Every medical drama is so good at showing the “‘ER’ doors slam open, gunshot something bleeding out, team jumping on chest, blood everywhere, ‘Call a code’ and so forth and so on….. but no one shows an on call doctor at 3am, clad in sweaty scrubs, theatre hat hanging off the neck, one scrub-cover shoe on, mask dripping with electrolytes and sweat (Bye sodium) struggling with a 27 weeker premature neonate with a glucose of 1.8, distended abdomen on CPAP. The pressure is building, your skills are fading, the crying/whimpering suddenly stops, lethargy- that you? One of these situations is more intense than the other, I feel.
Newborns are so vulnerable and deceptively unstable (and sometimes just evil). They have an incredible capacity to bounce back and fight disease but also get so sick so quickly. Everything in the NICU happens at light speed and if you’re slow enough, you miss most of it. Oxygen sats tanking, blood pressures in the boots, bed 3 forgot how to breathe (apnoea’s), ventilator alarms and monitors forever beeping..
And this is all before you’ve even entered the NICU and washed your hands.
I remember my very first NICU call, I was sweating because well, I was nervous and I felt like I had just stepped into a very crowded and noisy furnace. The temperature is controlled to keep the newborns warm and toasty, while we sweat our skin layers off slaving to their every need.
It was ridden with stress. I walked into the call with 3 babies on the ventilator- 2 relatively stable babies who were well behaved and 1 problem child (usual).
Besides having a clinically busy call, having an administrate busy call is far worse. It’s hard to begin a 24 hour call knowing the unit is maxed out without any bed space (A South African folklore).
Any new baby needing high care or ICU will automatically be a logistic problem on top of their trying-to-die problem which surprise, is indeed, both your problems. The feeling of I want to help save a life but also, in which bed? NICU nurses are absolute heroes. They’re so primed to notice any change from baseline, its uncanny. But once admissions with a full unit force you to shuffle babies around at odd hours which means moving around ill patients at 2am whilst admitting new patients with half the staff, everyone is obviously frustrated.
Before 4pm, I prayed deeply for no more unstable babies and admin issues.
God and the uteruses ignored me. Obviously.
Bed 1 was a tiny little 1kg fighter who had been in the unit for 2 weeks. he had attempted to die on multiple occasions but always bounced back. He was a problem child with overwhelming septic shock on triple inotropes and bilateral intraventrucular hemorrhages (IVH’s). He was day 10 on the ventilator and was due to be extubated soon. I made sure all his IV lines were functional and gave him small pep talk about no-evening-nonsense.
Bed 2 was a bigger 2,5kg baby with a pneumonia and what we suspected to be ongoing hospital acquired sepsis. I was waiting for a repeat FBC and any sign to upscale his antibiotics. I didn’t expect any serious trouble from him during the night.
Bed 3 was a 3kg baby with congenital syphilis. The mom had good clinic attendance and done everything right but happened to contract syphilis in her last trimester, from her partner who decided to have unprotected sex with various women. That selfish and careless act grated my last nerve and made my blood boil. I hoped the baby would only require a short and sweet ventilation to overcome her congenital pneumonia, while the antbiotics did its job.
I peered out into the high care domain, consisting of 12 babies who looked as stable as can be. Aside from the no-bed problem, they weren’t expected to be troublesome.
Shortly after, I had received a new admission from labour ward. A massive 3kg baby, fresh out the uterus. On eyeballing, he looked sick but i was hopeful it was just the -out of uterus look-. He was green- Meconium stuck to him like glue. The history i received was that the mom was a 39 year old femle, first pregnancy, difficult labour and fetal distress. They had managed to get the baby out with some generous episiotomy incisions (cringe) as she was too far along in labour to have a caesarean section. He was fine, until he wasn’t. Respiratory distress.
had he aspirated and choked on his own meconium (sterile poop)? and now the muck had collected in his lungs causing problems or was it just adaptive TTN?. He had no intrauterine problems and judging by his weight, he had thrived. He was obviously a precious pregnancy to an aged mother. We put him on 30% of oxygen and IV Fliuids and ran a blood gas. I watched his every breath, praying his breathing would slow down and his chest would stop recessing. I switched all unnecessary machinery off so I could listen to his breathing efforts while I said a silent prayer for the pa02 to be high on the blood gas.
My intern colleague stared at me from across the room and I just knew, he was hypoxic.
“the Pa02 is 5 Kpa”. Also look- his sats are dropping.
Sweat dripped into the corner of my mouth, a salty taste I am now quite familiar with.
Grabbed a CPAP machine and said nothing. The silence in the room made his grunting more obvious. I was stressed. I called for an urgent chest x-ray but I knew it wasn’t looking good. Meconium aspiration syndrome is just not something you can bullsh*t around with. MAS/PPHN/No Oscillator or nitric oxide. Trouble looming.
I called my boss and relayed the story. It was a no brainer-Ventilate the baby on bed 4 then try and find a bed in the outlying hospitals,a time consuming chore everyone dreads.
I made a mental note of everything I needed to do in the NICU: ventilate new baby and find an ICU bed somewhere, do PM gases and PM rounds on the babies already ventilated and tackle 3 drips in well baby nursery. My intern colleague joined me and we strategized. She started with the drips and I started with the ventilation.
Now, any new medical officer in the NICU will agree that intubations are scary at first. Taking control of a baby’s airway on your own is daunting. The 100’s of things can that possibly go wrong start popping up in your head and you feel like you’re crossing a minefield in clown shoes. Everything is so miniture and quaint. The laryngoscope blade, the endotracheal tube and ofcourse…. The vocal cords. Too much sedation? Too little? Pulmonary hemorrhage?
What if I can’t get the tube through the nasal passages? What if the laryngoscope light doesn’t work? What if I can’t find the vocal cords? What if I find the vocal cords and the tube wont go in? What if while im strapping the tube (the hardest part) the tube slips out? What if the tube is in, but too deep and I blow a pneumothorax? What if the hospital burns down before I get the tube in?
I shoved these doubts aside and found the precious cords fluttering, meconium oozed,. The moment of truth with my neck hyperextended glaring at the sats monitor- I looked at the monitor while I neo-puffed…68…wait….63…maybe, pulse 128…127….144… just maybe…sats… 68…69…my heart was pounding… 76…81….84….88….92…..95….. I felt a wave of relief the pressure around me slowly dissolved.
I realised I still needed to find a bed for this baby. I started the tedious job of calling 6 outside hospitals and prepared my generic speech. After an hour of calling and begging, a bed was found. (RKK to the rescue). I called EMRS and obviously, no ambulances were available. Grayyyt. I called the control room and spoke to the supervisor. My frustration was building. I made 9 calls looking for advanced life support teams, there were none. I had not reviewed anyone else and all my time was ticking away. Eventually, They assured me the baby could be airlifted with a helicopter. Choppers always excite me, my frustration was over.
I started my PM gases and reviews. Out of the corner of my left eye, I saw someone in green theatre garb moving around, that meant a new baby. My pulse was up again. I rushed to the receiving area and found a two-for-one special ie. Undiagnosed Prem Twins, In respiratory distress. The intern had attended the delivery and didn’t have time to let me know. I thought she was hydrating. I was wrong.
Premature twins at 800g and 900g both staring at me in severe respiratory distress. I stared back at them.
Where am I going to put them? theres no bed space. I started scouting high care for potential movers. Room air babies and fatties were at the top of my list. I moved 2 to well-baby nursery to make space for the twins.
They may need in-and-out surfactant, a substance to help the lung expand better. Maybe time will go slower now. I’m sure these were my only issues for the night. I’m sure God is done now.
We did the relevant investigations and consulted with the boss. Surfactant and CPAP. I hoped that would be enough.
Time was running and I hadn’t even started my PM gases and reviews on the ICU babies and the drips kept piling on (story of my life). I moved around like a headless chicken on steroids and got the gases done. While I waited for the results, I carried on with my reviews. Bed 2, 3 and new baby bed 4 were fine for now. We were waiting for the helicopter to arrive for bed 4 (felt cool to think that).
All of a sudden, Bed 1 looked suspiciously grey and dusky and his sats on the monitor read 89%. I manouvred the sats probe to another limb and checked his BP. I scanned his chest for movement and listenined for air entry. Everything seemed fine. Sats dropped to 86%. I shuffled nervously. Something sinister was cooking somewhere. My colleague returned with the blood gases and I looked at bed 1-low pa02, high pc02 and a Ph OF 7.0 (if you know, you know).
I felt the lump in my throat descend into my chest.
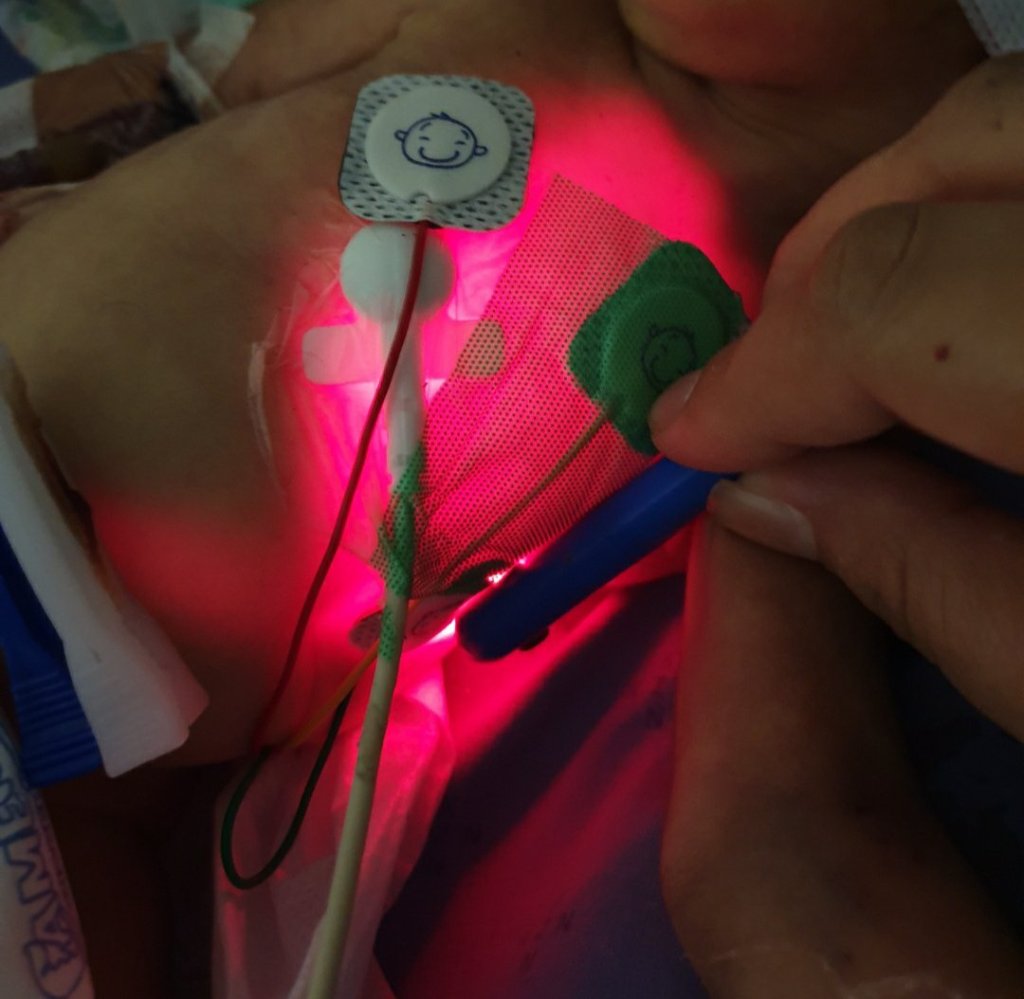
I grabbed the transillumintor and switched the lights off. I was convinced the baby had a pneumothorax.
The chest lit up like Christmas eve. No
My mind was buzzing but there was no time. prepped to put in the intercostal drain to drain the air which was squashing the lung. I knew I had to act quickly or else this would become a full on resuscitation- the worst possible scenario.
I pushed the drain in and saw the sats come up to 94%. Finally, something good was happening.
I sat down for 5 minutes and felt hunger, thirst and deep internal fatigue. The burden of the NICU surfaced in an instant. Every failed resuscitation, hours of dripping newborns with impossibly small delicate veins, failed intubations, months of growing 800grammers, trying to topple sepsis and losing almost every day. Why was this happening now? I threw myself a quick pity party before realizing morning is here and the work must go on.
I heard an unfamiliar sound above me and I knew, the chopper had arrived. This lifted my spirits. I welcomed the paramedic entourage in. We made some small talk about flying around and readied the baby. We connected the mobile ventilator and I scanned the sats monitor- 97%. Praise God. I waved them out and attended to the 2 new children, stable babies, thankfully.
I had a smile on my face. The morning was here, I was almost free from the clutches of the NICU. I started my 6 drips and counting. My eyes struggled to stay opened as I continued my search for veins within a radius of 1cm, the general theme of neonatology.
I looked up and saw a paramedic waiting for me. There are very few reasons he would return. Either he forgot his pen or the baby was unstable.
Please be the pen. Please be the pen. I reflexly handed him my pen.
“Doc, we have a problem. The mom is scared of flying. She refuses to get into the helicopter and there are no ambulances on the ground to take her to RKK…we have tried to convince her but she wont go”
Now I was panicking. The baby could not go without the mother. What milk would he drink? How would she get there on road with so few ambulances? What if he dies?
I speed walked outside and met *Mbali at the entrance. I saw her grip her abdomen in pain, barely post delivery, a mixture of tears and fear in her eyes. Blood trickled down her knee. I ushered her into the nearby bathroom and tried to help her clean up. She admitted she was in pain and had a fear of flying and had never flown before.
“its not that I don’t want to doctor, its that I am so afraid”
I held her hand and hoped she felt the same fear I had felt throughout the night.
“Mbali, Your baby really needs to go to Durban now. He needs you. I know you’re scared and I don’t know whats going to happen in the helicopter. But I do know what will happen if your baby does not go to ICU”
It didn’t take much convincing before she was looking down on me as the heli took flight. The fear in her eyes still very present.
There’s something just so extrateresterial about a mothers love for her child. It transcends fear, law, logic, risk and boundries. I have come to realize the power and depth of a mothers love on countless occasions in the NICU. That deserves a separate post altogether.
Watching Mbali fly away despite her fears, helped me face mine that night. My deep thoughts were interrupted by My phone ringing, theatre had a Caesar for fetal distress with meconium exposure. Let the literal sh*t show commence again, I thought.
I remembered the paramedic had taken my pen. Luckily it was A Bic. I borrowed a pen from a sister who borrowed it from an intern who said she found it in theatre. It had a broken nib and a chewed off back.
I limped back to NICU like an injured lion armed with my defective pen, back on the prowl. I knew the next 6 hours would be grueling but if a Mbali could show such courage, so could i.
I ended the call physically broken with a total of 8 admissions, 1 ventilation, 1 intercostal drain, 2 in-and-out surfactant and endless drips on my 1st call. The start to many flame-throwing, adrenal-squeezing, action packed calls that I have now come to somewhat enjoy (mildly).

You are incredible! 💛 Love reading your posts.
LikeLike
Enjoyed reading your posts. You are a hard worker and a life saver
LikeLike
Wow ! I’m hooked 😁
LikeLike
Wow Sabeeha. You have such an amazing talent… Took me right back to our NICU to the point where I got palpitations halfway through this post and scrolled right to the end to see if it all ended well before calming myself and going back to read the rest😂😂😂😂😂😂. Please write a book as well! Am sure it will fly off the shelves!
LikeLike
This is the first of your posts that I have decided to read. Your story is truely inspirational. I read the entire post with my breath caught in my chest! As a foreign medical graduate fresh off the board examination and a soon to be intern, I hope to take on future challenges just as you have. May Allah Ta’Allah take you from strenght to strenght, Ameen.
Can’t wait to read more.
LikeLike
Thank you so much for navigating to my blog and offering so much support! I was in a busy, overwhelming call and I saw all the support, likes and comments and it gave me courage. I wish you everything of the best on your journey/rollercoaster that is to come! Enjoy it and meet it with as much positivity and gratitude as you can- it helps!
LikeLike
Thanks so much the info.
LikeLike